A coccyx fracture involves a break in the tailbone and typically causes severe, persistent pain that takes 8-12 weeks to heal. A bruised coccyx (contusion) is soft tissue damage around the bone that produces moderate pain and heals within 4-6 weeks. An X-ray is the only reliable way to distinguish between the two, as symptoms overlap significantly.
By Dr. Emma Clarke | Physiotherapist & Pain Management Specialist | Last updated March 18, 2026
The coccyx — commonly called the tailbone — is the small, triangular bone at the very bottom of your spine. It sits below the sacrum and is made up of three to five fused (or semi-fused) vertebral segments. Despite its small size, the coccyx plays a surprisingly important role in your daily life.
The coccyx serves as an attachment point for several muscles, tendons, and ligaments, including portions of the gluteus maximus, the pelvic floor muscles, and the sacrococcygeal ligaments. It also functions as a weight-bearing structure — when you sit down, your body weight is distributed between your two ischial tuberosities (sit bones) and your coccyx. This is why coccyx injuries cause such significant pain during sitting.
The coccyx is connected to the sacrum above it by the sacrococcygeal joint, which allows a small degree of flexion and extension. This mobility is particularly important during childbirth, when the coccyx moves backward to widen the pelvic outlet. However, this same mobility makes the coccyx vulnerable to injury — it can be pushed beyond its normal range of motion by a fall, a direct blow, or the pressures of labour and delivery.
Understanding this anatomy helps explain why both fractures and bruises in this area can be so painful. The coccyx is surrounded by relatively thin tissue, sits close to the skin surface, and bears weight during one of the most common human activities — sitting. Even a minor injury here can produce disproportionate discomfort.
Coccyx injuries — whether fractures or bruises — share many of the same causes. The mechanism of injury can sometimes hint at whether you are more likely to have a fracture or a bruise, though this is not always reliable.
The most common cause of coccyx injury is a backwards fall onto a hard surface. Slipping on ice, falling from a chair, or losing your footing on stairs and landing on your buttocks can all deliver a direct impact to the tailbone. High-energy falls (from height, at speed) are more likely to cause a fracture, while lower-energy falls onto softer surfaces more commonly produce bruising. However, even a seemingly minor fall can fracture the coccyx if the angle of impact is direct.
During vaginal delivery, the baby's head passes through the pelvic outlet and can place extreme pressure on the coccyx. This can cause the tailbone to fracture, dislocate, or bruise. Difficult or prolonged deliveries, large babies, and instrumental deliveries (forceps or ventouse) increase the risk. Studies suggest that coccyx injuries during childbirth are more common than previously recognised, with some estimates indicating that up to 10% of women experience coccyx pain following delivery.
Contact sports such as rugby, football, and ice hockey carry a risk of direct impact to the coccyx. Cycling — particularly on hard saddles or rough terrain — can cause repetitive microtrauma to the tailbone area. Rowing, horseback riding, and certain gymnastics movements can also stress the coccyx. In athletes, the line between a bruise and a stress fracture can be particularly difficult to distinguish without imaging.
Not all coccyx injuries are dramatic. Prolonged sitting on hard surfaces — particularly with poor posture — can gradually irritate and damage the coccyx and surrounding tissues. Office workers, lorry drivers, and people who sit for extended periods on hard benches or chairs are at increased risk. This type of injury more commonly produces bruising or inflammation rather than a fracture, but chronic repetitive strain can weaken the bone over time.
Any direct blow to the tailbone area — a kick, a collision, or impact with a hard object — can cause either a fracture or a bruise depending on the force involved. In clinical practice, higher-energy impacts are more likely to produce fractures, while moderate impacts tend to cause contusions.
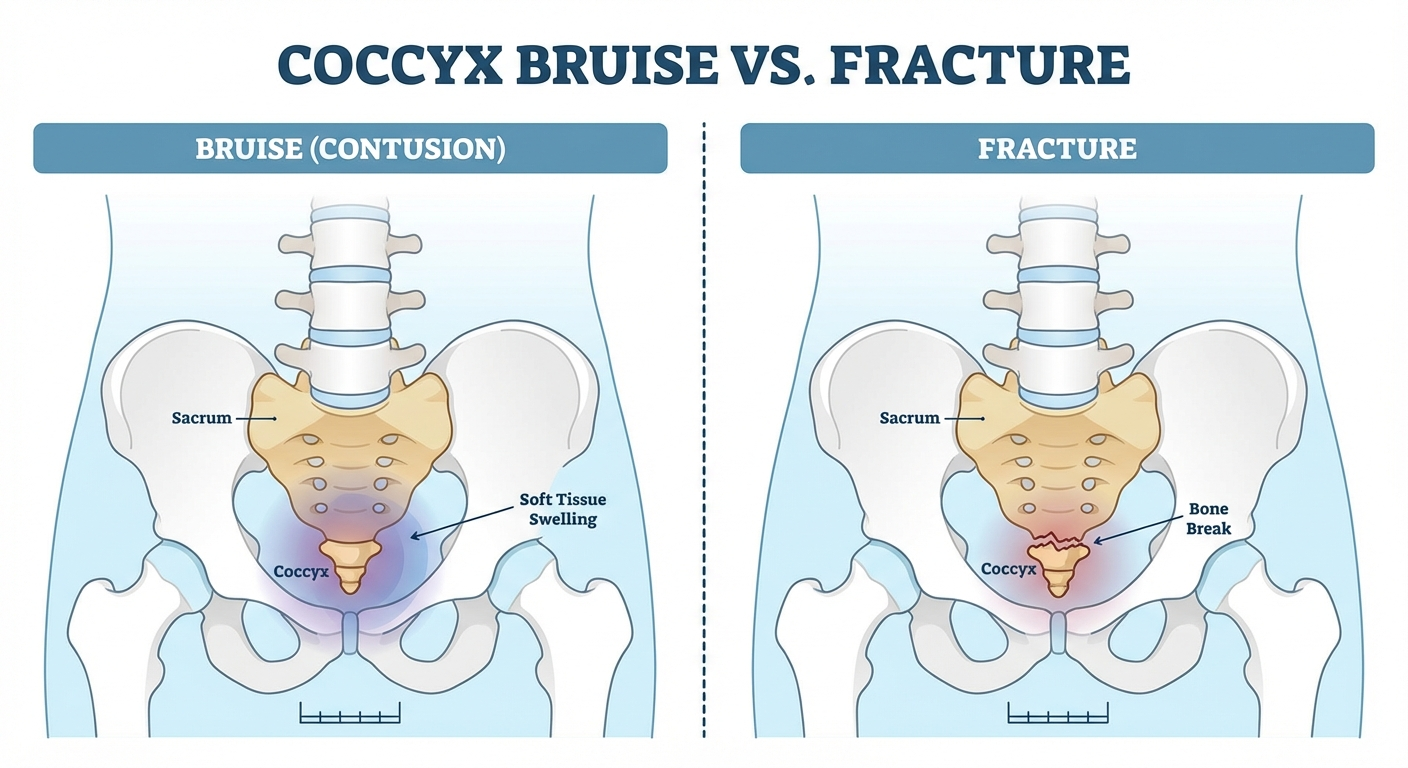
A bruised coccyx (coccygeal contusion) is a soft tissue injury — the bone itself is intact, but the surrounding muscles, ligaments, and periosteum (the thin tissue layer covering the bone) are damaged. Bruising can range from mild to severe, and symptoms can overlap significantly with those of a fracture.
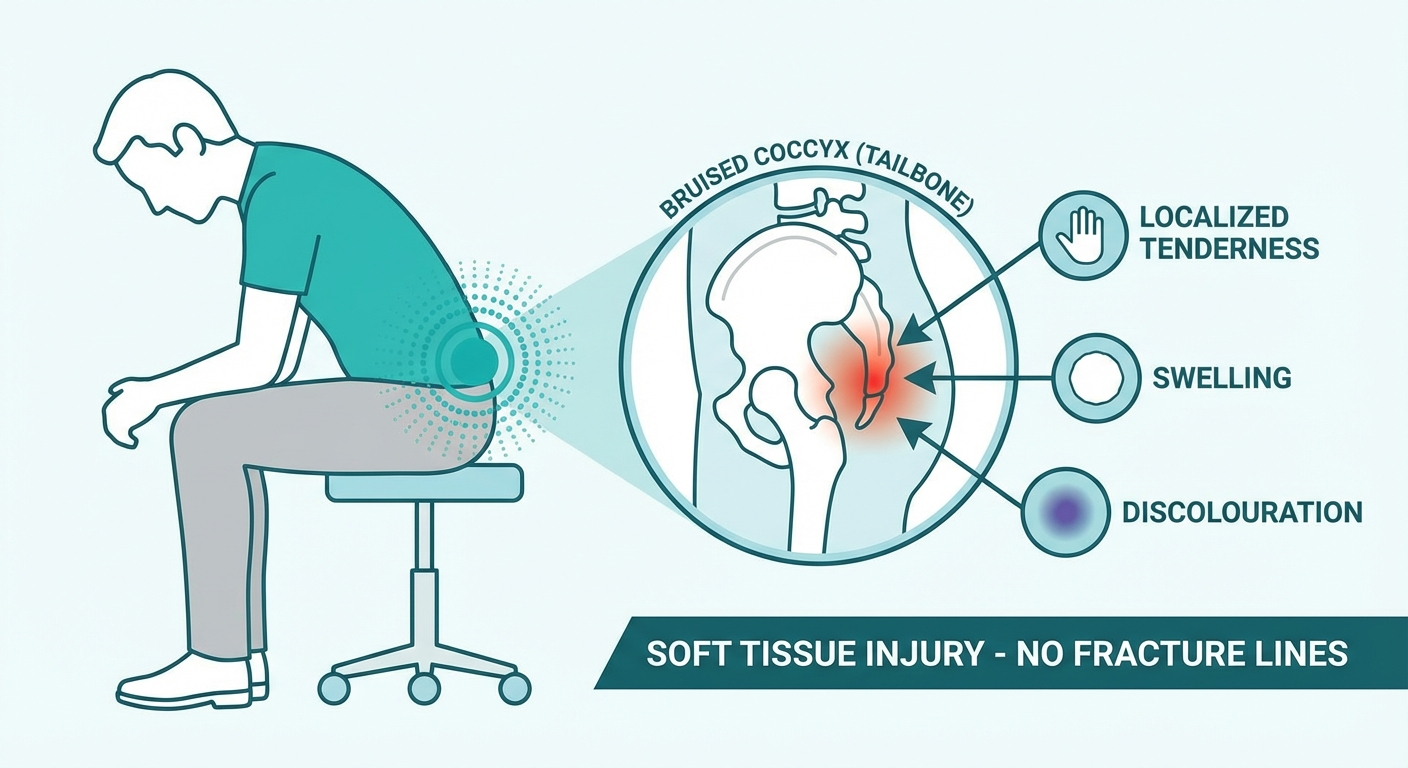
Bruises vary in severity. A mild contusion may cause only minor tenderness when sitting on hard surfaces, resolving within 2-3 weeks. A severe bruise — with significant soft tissue damage, deep haematoma, or periosteal bruising — can produce pain that is nearly indistinguishable from a fracture and may take 6 weeks or longer to resolve fully.
A fractured coccyx means the bone itself is cracked or broken. Coccyx fractures range from hairline (stress) fractures to complete breaks, and in some cases the fractured segment can become displaced or angulated. The symptoms of a coccyx fracture are often more intense than those of a bruise, but there is considerable overlap.
The following table summarises the typical differences between a coccyx fracture and a bruise. Remember that individual cases vary, and this table is a guide — not a diagnostic tool.
| Feature | Bruised Coccyx | Fractured Coccyx |
|---|---|---|
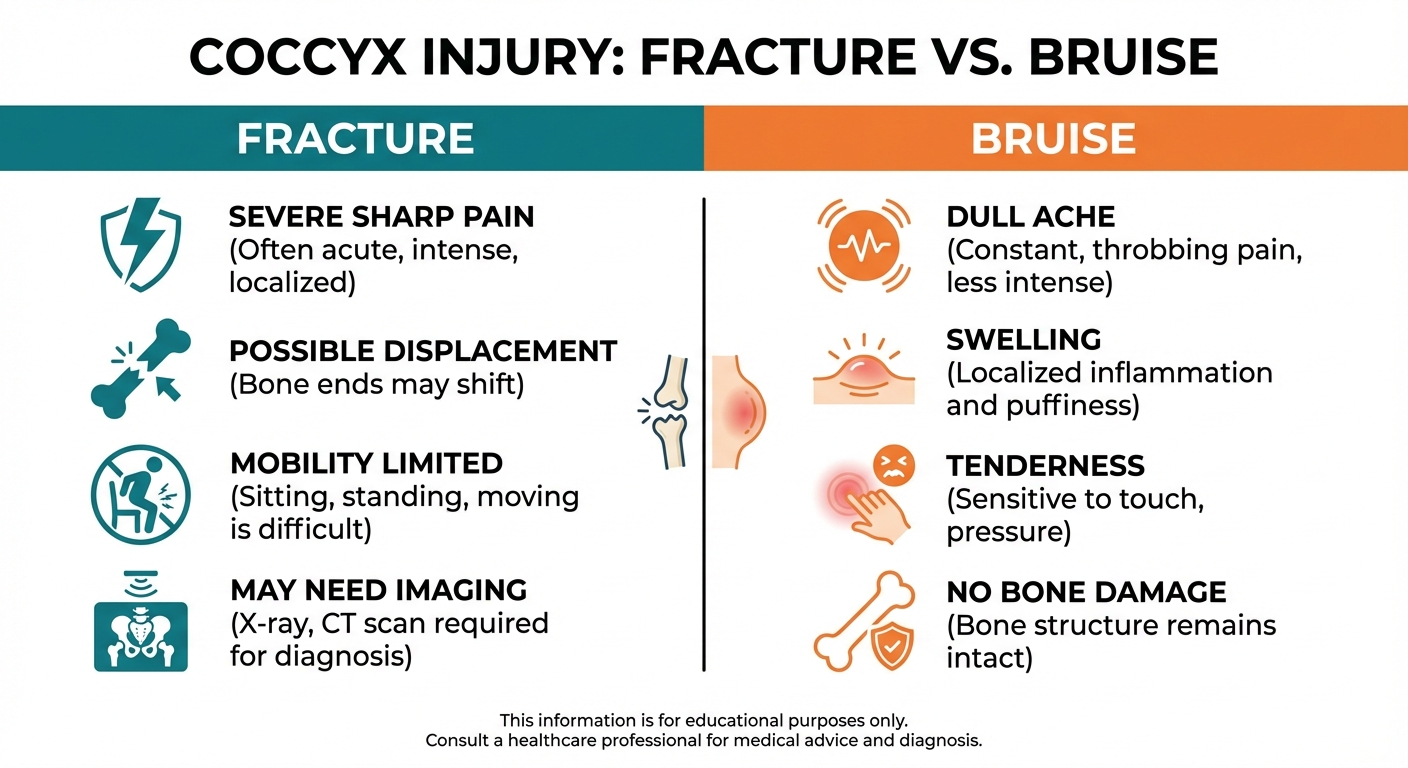
| Pain Intensity | Moderate — uncomfortable but manageable | Severe — often debilitating |
| Pain Trajectory | Gradually improves week by week | May plateau or worsen in the first 2-3 weeks |
| Swelling | Mild to moderate | Moderate to severe |
| Visible Bruising | May or may not be present | Often present and more extensive |
| Deformity | None | Possible palpable step or abnormal prominence |
| Sitting Ability | Painful but possible with cushion | May be unable to sit even on soft surfaces |
| Pain with Coughing/Sneezing | Mild | Often significant |
| Recovery Time | 4-6 weeks | 8-12 weeks |
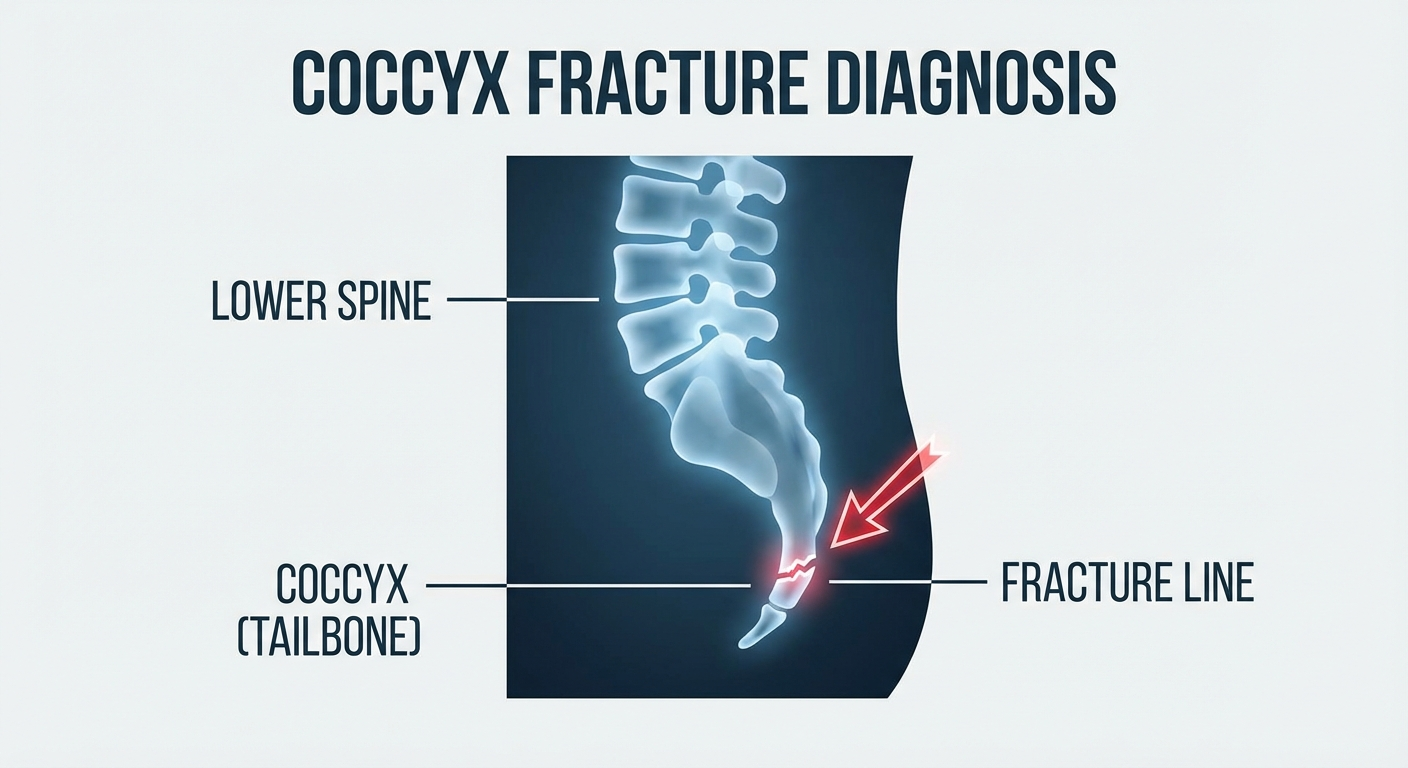
| X-ray Findings | Normal bone appearance | Visible fracture line, displacement, or angulation |
| Treatment Approach | Conservative (rest, cushion, OTC pain relief) | Conservative in most cases; rarely requires surgery |
Not every coccyx injury requires a doctor's visit. Many mild to moderate bruises resolve on their own with simple home treatment. However, certain circumstances warrant professional evaluation.
Your doctor will take a detailed history of how the injury occurred, the nature and severity of your symptoms, and any aggravating or relieving factors. They will perform a physical examination, which typically involves palpating (pressing on) the coccyx externally to assess tenderness, swelling, and any deformity. In some cases, your doctor may perform a rectal examination to assess the coccyx from the front — this allows them to feel for fracture displacement or abnormal mobility and is considered the most accurate clinical test for coccyx fractures, though it is not always performed.
Clinical examination alone cannot reliably distinguish between a coccyx fracture and a bruise. Imaging is the key to an accurate diagnosis.
A plain X-ray of the coccyx is the first-line imaging study and the most commonly used tool for diagnosing coccyx fractures. X-rays can reveal fracture lines, displacement of bone fragments, and abnormal angulation of the coccyx. Your doctor will typically request lateral (side-view) X-rays of the coccyx, as this view provides the clearest visualisation of the tailbone.
It is worth noting that X-rays have limitations. The coccyx is a small bone surrounded by soft tissue and overlapping pelvic structures, which can make subtle fractures difficult to see. Additionally, the normal anatomical variation of the coccyx — some people have naturally curved, angulated, or fused coccygeal segments — can make interpretation challenging. Despite these limitations, X-ray remains the standard diagnostic tool and is sufficient for the vast majority of cases.
If the X-ray is inconclusive but a fracture is strongly suspected, your doctor may order a CT (computed tomography) scan. CT provides much more detailed cross-sectional images of the bone and can identify hairline fractures, small avulsion fractures, and subtle displacements that standard X-rays may miss. CT is particularly useful for complex injuries or when surgical planning is required.
MRI (magnetic resonance imaging) is not typically needed to diagnose a coccyx fracture — X-ray or CT is usually sufficient. However, MRI is valuable when the doctor wants to assess soft tissue damage, rule out other causes of coccyx pain (such as tumours, cysts, or infections), or evaluate bone marrow oedema (a sign of bone bruising or stress reaction that does not show on X-ray). MRI may be ordered if pain persists despite normal X-ray findings, to look for occult (hidden) fractures or soft tissue pathology.
A bone scan (nuclear medicine scintigraphy) is rarely used for coccyx injuries but can be helpful in identifying stress fractures or other bony pathology when other imaging is normal. This involves injecting a small amount of radioactive tracer and scanning for areas of increased bone activity.
A bruised coccyx is treated conservatively, and the vast majority of cases resolve fully with time and simple self-care measures. The goal of treatment is to manage pain, minimise irritation, and allow the body to heal naturally.
Perhaps surprisingly, treatment for a fractured coccyx is often very similar to treatment for a bruise — because there is no practical way to immobilise or cast the coccyx. You cannot put a tailbone in a plaster cast. Treatment focuses on pain management and protecting the area while the bone heals naturally.
Surgical removal of the coccyx (coccygectomy) is considered only when all conservative measures have failed over a period of several months. Fewer than 10% of coccyx fracture patients ever require surgery. Coccygectomy has a variable success rate and carries risks including infection, wound healing problems, and pelvic floor instability. It is considered a last resort.
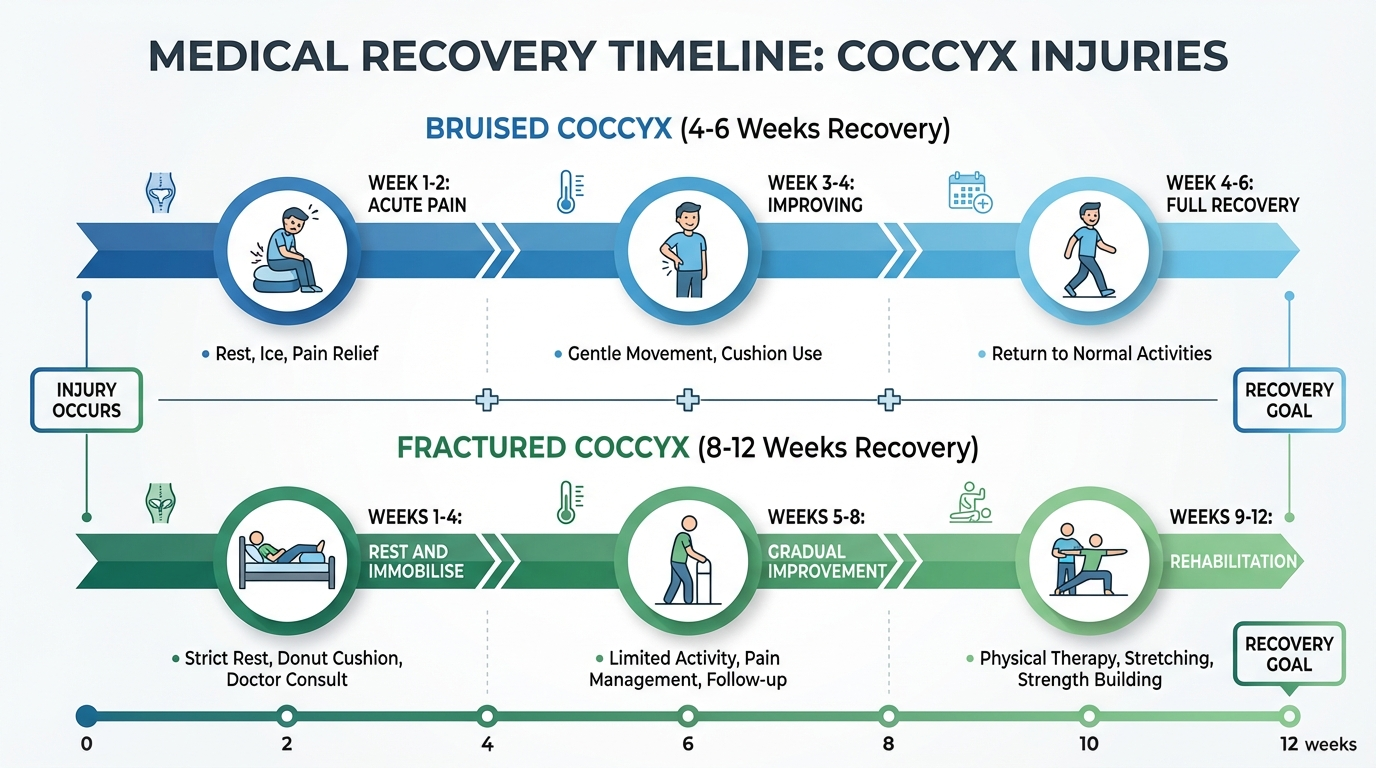
Recovery from a coccyx injury requires patience. Both fractures and bruises heal gradually, and attempting to rush the process by returning to full activity too soon often causes setbacks. Below is a typical recovery timeline for each injury type.
Whether you have a fracture or a bruise, day-to-day pain management is the biggest challenge during recovery. Here are the strategies I recommend most frequently to patients.
A coccyx cushion with a rear cutout is the single most impactful change you can make. It removes direct pressure from the tailbone and can transform sitting from agonising to manageable. Use it everywhere — at your desk, in the car, at the dinner table.
Lean slightly forward when sitting to shift weight onto your thighs and ischial tuberosities rather than your coccyx. Alternating between sitting and standing every 20-30 minutes also helps. Consider a supportive office chair if you work at a desk.
Apply ice for the first 48-72 hours, then switch to heat. A warm bath before bed can be particularly helpful for relaxing pelvic floor muscles and improving sleep quality during recovery.
Sleeping on your side with a pillow between your knees reduces pressure on the coccyx and keeps your pelvis aligned. Avoid sleeping on your back if it causes tailbone pain. A firm mattress tends to be more comfortable than a soft one for coccyx injuries.
Gentle walking is one of the best things you can do during coccyx recovery. It promotes circulation, prevents stiffness, and supports mental wellbeing. Avoid high-impact activities, heavy lifting, cycling, and rowing until your pain has resolved.
Our expert-curated relief programme includes cushion recommendations, exercise guides, and step-by-step recovery plans tailored to your injury.
Get Your Relief Plan →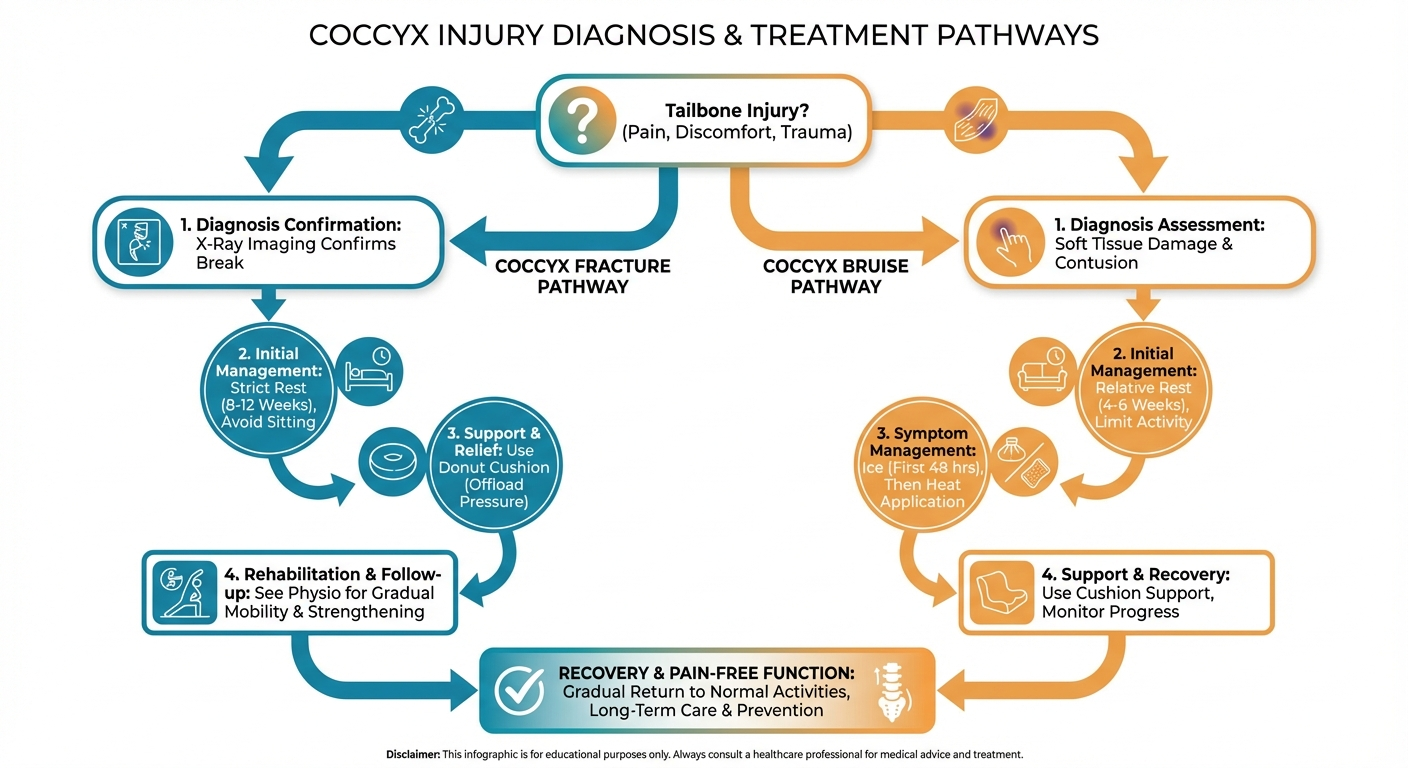
You cannot definitively distinguish a coccyx fracture from a bruise based on symptoms alone — an X-ray is the only reliable way to confirm a fracture. However, fractures tend to cause more intense pain, visible deformity or swelling, pain that worsens or plateaus over weeks rather than improving, and difficulty sitting even on soft surfaces. A bruised coccyx typically produces moderate pain that gradually improves within 2-4 weeks.
A bruised coccyx typically takes 4 to 6 weeks to heal with conservative treatment. Most people notice significant improvement within the first 2-3 weeks. During recovery, use a coccyx cushion when sitting, avoid prolonged sitting, apply ice for the first 48-72 hours followed by heat therapy, and take over-the-counter pain relievers as needed.
A fractured coccyx typically takes 8 to 12 weeks to heal, though some fractures may take longer depending on severity, the patient's age, and overall health. Some patients experience residual tenderness for several months after the fracture has healed. During recovery, follow your doctor's guidance on activity modification, use a coccyx cutout cushion, and attend physiotherapy appointments as recommended.
An X-ray is recommended if you experienced significant trauma (such as a hard fall), if your pain is severe and not improving after 1-2 weeks, or if you have signs suggesting a fracture such as visible deformity, inability to sit, or pain that worsens over time. For mild tailbone pain after minor incidents that is clearly improving, an X-ray may not be necessary — your doctor can advise based on your specific situation.
Yes, most coccyx fractures heal on their own with conservative treatment. There is no cast or splint that can be applied to the coccyx, so treatment focuses on pain management, activity modification, and allowing the bone to heal naturally over 8-12 weeks. Surgery (coccygectomy) is only considered in rare cases — fewer than 10% — where the fracture fails to heal after several months of conservative care.
Seek emergency care if you experience bowel or bladder dysfunction, numbness in the saddle area (inner thighs, groin, buttocks), progressive leg weakness, fever alongside tailbone pain, or if the injury resulted from a high-energy trauma such as a car accident or fall from height. For moderate tailbone pain after a fall, booking an urgent GP or physiotherapy appointment within a few days is usually appropriate rather than visiting A&E.
Gentle walking is encouraged throughout recovery for both bruises and fractures. Avoid high-impact activities, cycling, rowing, and heavy lifting until your pain has resolved. After the initial acute phase, your physiotherapist may introduce gentle stretching and pelvic floor exercises. Pilates-based exercises can be beneficial for coccyx recovery once your pain has settled to a manageable level — typically after 3-4 weeks for a bruise and 6-8 weeks for a fracture.
This guide is based on current evidence-based practice guidelines for coccyx injury assessment and management, combined with clinical experience treating patients with coccydynia. Recommendations align with protocols from the NHS, the American Academy of Orthopaedic Surgeons, and peer-reviewed physiotherapy literature.
Key references consulted:
Content has been reviewed for medical accuracy and reflects standard clinical practice as of March 2026. This article does not constitute medical advice — always consult a qualified healthcare professional for diagnosis and treatment of coccyx injuries.
Related reading: Cold vs Heat Therapy for Coccyx Pain | Coccyx Pain & Sitting: How Long Is Too Long? | Best Coccyx Cushions 2026 | Best Office Chairs for Coccyx Pain | Can Pilates Help Coccyx Pain?